I had forgotten what simulacra Level 1-4 simulacra mean. Here is a link for anyone else that had also forgotten.
Level 1: “There’s a lion across the river.” = There’s a lion across the river.
Level 2: “There’s a lion across the river.” = I don’t want to go (or have other people go) across the river.
Level 3: “There’s a lion across the river.” = I’m with the popular kids who are too cool to go across the river.
Level 4: “There’s a lion across the river.” = A firm stance against trans-river expansionism focus grouped well with undecided voters in my constituency.
1. Truth
2. Lies/Influence
3. Bullshit*/Appearances/Social Lies
4. People are Twitter bots
*No reality connection
I think disagreement about herd immunity comes down to whether we're talking about "herd immunity despite everyone going back to clubbing and indoor dining etc. as if it were 2019" vs "herd immunity while cautious people continue to take COVID-19-specific precautions". I think the population heterogeneity is very high under current conditions, where lots of people are all but entirely isolated, and that the population heterogeneity is quite a bit lower under normal circumstances, where more isolated people sometimes go drink tea with their highly social neighbors and family members etc. When people hear the words "herd immunity" I think they're usually imagining that we all get to go back to 2019 behavior, but I don't think you're using the term that way. You can correct me if I'm wrong.
I did a little digging on schools staying open in Europe and I suspect the decision to keep schools open in Europe has been partly driven by this paper from the ECDC (dated 6th August) which suggests the attack rate in schools is low.
They base this on:
- Some contact tracing investigations (I think ~6 total) from schools, most of which showed at most 1 onward infection. However they note one study of an Israeli school where 2 index cases ended up being 178 cases in the school and more in the community.
- Countries which reopened schools without noticeably increasing R and without significant school outbreaks
I do think there is some bias towards wanting to keep schools open (I think they downplay a couple of papers which suggest schools could be causing more infections) but actually the evidence is better than I expected. Of course they could be leaving out other studies completely and I wouldn't know.
Regarding the cough identifying AI: Due to the online collection method I suspect that most of the positive samples were already quite advanced in their disease progression. Since Covid-19 deposits in the lungs mainly in the latter part of the disease it is easier to identify them at that point, but also not that useful anymore because most of the transmission happens during the earlier part of the infection (both for symptomatic and asymptomatic people).
These researchers had a much better sample procedure, cough samples were mostly acquired at testing sites, where participants did not know yet whether they have Covid (much less risk of subconscious bias) and were presumably at an earlier stage of their disease. They also had much worse results, which I suspect are more realistic for a real world setting.
What actually needs to be done is to do a longitudinal analysis, i.e. you record your baseline cough when you are healthy. Then if you want to check if you are infected, you cough again and compare that "potentially sick" cough against your baseline "non-covid cough". The potential of this approach is much higher since baseline characteristics of the cough can be accounted for (smoker, asthmatic, crappy mic in phone).
I have been thinking that it should be possible to gather training data for this quickly by identifying a subset of people that are somewhat likely to get sick in the near future like e.g. people participating in big parties, and acquire coughs from them prior and subsequent to infection. If somebody has ideas how to acquire such data, feel free to share. As an aside, I am somewhat surprised that we as a community interested in AI and out-of-the box thinking have not focused/discussed AI for Covid detection much earlier.
I continue to be very confused that major European countries are keeping schools open while otherwise locking down, but don’t have anything useful to add on that subject.
Months ago I heard that kids are more resistant to COVID-19, not sure if this is still considered true.
The reason to keep small kids at school is that otherwise one parent needs to stay at home with them. If you close schools, a large part of population cannot work anymore. Presumably those countries want to avoid the economical consequence of this.
I am explaining the policy here, not defending it. I suspect that when a large part of population gets into hospitals, it will be worse than merely having them stay at home with kids. But perhaps people feel that the cure will come soon, or the exponential curve will stop being exponential, or simply most people only care about short-term consequences.
In Germany, one reason for keeping older kids at school is the fear that underprivileged children would be disadvantaged by distance learning (not having the necessariy technology, not having a quite room for themselves, having less parental support) thereby further widening social disparities in school outcomes that are already being seen as highly problematic without that effect.
(I am explaining the policy here, not defending it.)
I do hear similar arguments a lot. It's a hell of a reason to not deal with a pandemic, but that's where we are.
An interesting question is what leads to this kind of reasoning?
Of course, in theory it could be a set of preferences, assigning a very high value to the learning chances of underpriviledged groups compared to the health of mostly elder people. But that is not very likely because in that case this quite extreme set of preferences should manifest itself in other political decisions, too. Which it doesn't.
I suppose it is a little bit of magical thinking - implicitly thinking the virus can be negotiated with, if the goal of a public policy is worthy enough.
Regarding Germany, masks, and Dr. Lauterbach's 75%:
I wouldn't put too much trust in the 75% figure by Dr. Lauterbach. He has used that exact figure since as early as March 2020 on twitter - mask wearing has become obligatory in many areas of public life at the end of April 2020 in Germany. Dr. Lauterbach (epidemiologist and politician) is probably the most hardline politician when it comes to fighting Covid in Germany (not a bad think from my perspective) so I think your remarks about Dr. Fauci and the Simulacra Level 2 apply to him, too.
And from what I am seeing mask compliance and social distancing in the public in Germany are quite high. E.g. I can't remember having seen any customer in a grocery store without a mask for the last 6 months. On the public transport systems, too, the mask compliance seems to be quite high. And there are fines if you don't comply, and they have been in place for months.
Here are parts of a press release by the public transport system of one of Germany's metropolitan areas (Rhein-Main, Frankfurt) describing mask wearing checks since mid August, i.e. even at a time when the subjective threat level was quite low in Germany (ca. 1,000 diagnosed infections per day in Germany):
"50 days after the start of the campaign, the team has encountered more than 300,000 passengers. The result: Less than one percent of all passengers were travelling completely without any mouth and nose cover. A further almost 7 percent wore their cover incorrectly, for example under their noses. More than 88 percent of all passengers without or with incorrectly worn masks complied, corrected the fit of their mouth-nose-covering or accepted a mask from the prevention team.
The rate of mask refusers was less than one percent over the entire period. However, the number of passengers with incorrectly worn masks fell from just under seven percent to a good five percent over the course of September on regional rail services, for example." RMV.DE
I think where social distancing and mask wearing hasn't worked the last months are two specific areas: private life (including large weddings or funerals) and schools. In many parts of the school systems it was believed possible to stop forcing the students to wear masks after the summer. Not such a good idea. And the German school bureaucracies are the less efficient parts of the civil service, quite dysfunctional in some German states while the local schools in many cases don't have the autonomy to decide for themselves to do more when it comes to infection prevention.
The post about Sweden's unusual situation you linked to has updated. The author claims that the reduced death rate is mostly due to younger people getting near all of the covid cases, which is supported by recent data (the figure shows total number of changes between July and 03 Nov). Why that is the case is another issue.
Edit: As always, thanks for the post.
It sounds like your 400k deaths median is "until herd immunity", but then there's a period where R < 1 but because people are currently infected it takes time for the virus to die out, even assuming no behavioral changes. Do you have a model for how long, and how many deaths, that later period takes?
I feel like the herd immunity section is overly simplistic given how much IFR varies based on age group.
Using https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v7
The estimated age-specific IFR is very low for children and younger adults (e.g., 0.002% at age 10 and 0.01% at age 25) but increases progressively to 0.4% at age 55, 1.4% at age 65, 4.6% at age 75, and 15% at age 85.
65+ is like 45,000,000 in the US. Half of them get infected, generously let's say 3% die that's 600,000 dead. A big part of the IFR in the spring for NYC and Sweden(and probably lots of other places) was determined by the virus getting into care homes or not.
This being said I am leaning towards herd immunity being a decent solution with 2 major caveats:
1. You really need the 65+ demographic to stay reasonably locked down while you're burning through the rest of the population. And for countries where multiple generations are living together that's not possible. And for countries where a ton of older people don't worry about the virus that's also not possible.
2. You can't variolate(?) too quickly, otherwise you just blow out your hospital system and suddenly those nice 0.4% death rates blow up into ?? who knows.
Briefly looking for estimates of hospitalization rates I found https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7493765/
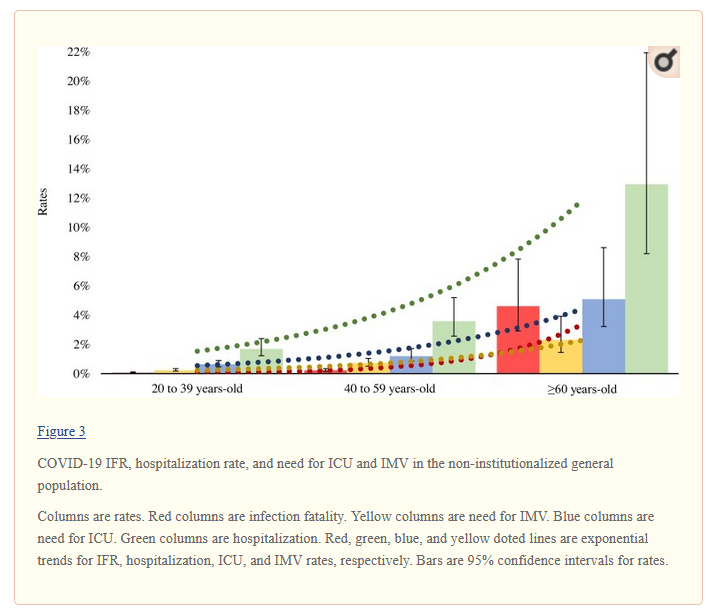
I'm super worried about Europe, because I think several countries are going to get pushed to medical system collapse and beyond. Assuming the study above is reasonably representative, let's say 4% of 40-59 year olds are admitted to hospital, based on the graph above(a group with an IFR of like 0.2%). If the hospital is full what percentage of people that needed to be admitted dies? Does he IFR go up x3? x5?
Was hoping to visit my family in Romania for the holidays, but at this stage I'm probably hunkering down in good old blighty til spring :(
EDIT. Basically I think the situation for herd immunity is both better and worse than what I derive from your post: The IFR for the groups of people we want to get the disease is well below 0.4% on average. But we REALLY want at risk groups to be in close to lockdown mode while variolating.
As an extra wrinkle, viral load seems to have a significant effect on disease severity. If a country is purposefully going for herd immunity, at the peak of the process viral load in closed spaces will be a lot higher than it is these days. That may or may not shift IFR higher for a while.
Mutation has always been an elephant in the Covid-19 room, and I haven’t paid as much attention to it as I should have. It is increasingly clear the Covid-19 has mutated, and the new strain is substantially more infectious than the old one and now virtually the only strain. One write-up from the Financial Times: Scientists warn a more infectious coronavirus variant spreading across Europe. The new strain doesn’t seem different from the old one once you are infected, in terms of your prognosis or chance of death, and immunity to either strain gives immunity to both.
I remember being told the new version was ‘ten times more infectious’ but I can no longer find the reference, and in any case case who knows what such phrases actually cash out into in terms of magnitude, what the new baseline R0 is, or how much we would need to tighten our precautions to compensate. If you do know, please let us know. My assumption is that the change probably cashes out to not that big a difference in practice, and likely a misleading way to categorize what’s happening, but I have no idea.
What I do know is that it makes sense that if your previous goal was to do exactly enough to keep things under control, or your people were using control systems to do the same thing, and then the virus gets more infectious, you are going to be in a lot of trouble until you can adjust. Especially if winter arrives at the same time. And adjusting sufficiently won’t be easy.
This also throws a wrench into any calculations regarding herd immunity. Previously I was confident that 50% immunity, if accumulated through uncontrolled spread, would be more than sufficient. If the baseline R0 is suddenly much higher, that could no longer be the case. How much not the case depends on the magnitude of the change. Again, I do not have a good read on that.
I also suspect, both due to dropping death rates (which likely have multiple compounding causes) and also purely on first principles, that the new strain is effectively less deadly. Initial viral load when infected likely matters for how often you die and how bad your prognosis is in general. If the new virus is more infectious due to things like changes in its spike proteins, but replicates at the same rate and is equally vulnerable to an immune system response once it starts, it seems likely that it results in lower average initial viral loads. That in turn would make it effectively less deadly, even if a laboratory test would indicate no difference. I’m curious what other people’s takes on this might be.
Aside from Covid-19, nothing else important happened this week. Let’s run the numbers.
They’re not good.
The Numbers
Deaths
Things continue as we might have expected, with another steady rise in the death rate especially in the Midwest. There are some details worth pointing out that don’t make it onto the graph or chart.
In particular, the rise in deaths was entirely in the last three days and especially in the final day, when deaths jumped to 1,566 at the same time positive tests first exceeded 100k. That’s 300+ more deaths than any day in the past few months. This raises my fear of a rapid acceleration from here, but the most likely explanation is that everyone was busy or distracted, intentionally or unintentionally, and shifted their reporting forward in time a bit, underreporting earlier and catching up now. It is clear that test and death counts reported on a given day are somewhat correlated due to variance in how much data the system can process on any given day.
Also, some unusually large irregularities out West mostly cancelled out, as Arizona had a dramatic rise in deaths while California took a plunge. I don’t expect either effect to be sustained.
Test Counts
Positive Tests
Positive test percentages are rising and were especially high yesterday, so if anything the number of cases is rising faster than this. The rise looks more dramatic on the graph because it is a percentage rise off a high baseline and that’s how exponential growth works. This is the baseline scenario of cases continuing to rise at the same pace until deaths rise enough to case behavior adjustments, and/or we do major lockdowns that I don’t expect.
Positive Test Percentages
There was a huge and quite scary jump in the midwest. Other regions continue to get steadily worse, and on slowly improving test counts. We see no signs that this weave is about to peak, and testing is not expanding fast enough to keep pace. My model is that even when testing looks fully adequate the majority of cases are never identified. When positive test rates are double digit, I believe the vast majority of cases are being missed.
Nothing in the sections below is as important as the numbers. We have uncontrolled spread almost everywhere, growing by double digit percentages on a weekly basis, and we don’t yet see signs people are adjusting behavior or any sign of the political will to impose measures sufficiently effective to work.
I hope that we are only a few weeks from things turning around due to behavior adjustments, despite not yet seeing any sign of those adjustments. There are reasons for optimism and hope, but for now that’s all that is. Hope.
Europe
(That spike in Spain is them adding in past deaths, so ignore it.)
Lockdowns are in effect in many places across the continent. It takes some time to see the benefits in infections, and several weeks more to see the death rate decline. When you first lock down, there is a brief period where in-household infections actually accelerate even as out-of-household ones decline. Next week will get us past that stage, so we’d better start seeing these infection curves turn sharply downward. If they don’t, then either lockdowns will need to tighten further or defeat will need to be conceded. There aren’t any other options.
Sweden’s death rate is going down again. I don’t have a theory or a story to tell, but it’s curious.
Well, Belgium
Belgium seems to have it worst of any country in Europe. It’s bad enough I pulled them from the graphs because adding them changed the Y-axis and made the graphs harder to read – you can play around with the data site here. According to this interview, the medical system is expected to collapse within a week, although things could be sustained longer if patients can be diverted to Germany or other nations. The numbers here are scary as hell. If the source is correct, 25% of doctors are symptomatic right now. The number infected is that much higher, and this is after having a reasonably bad but quick first wave. Doctors known to be positive are working anyway, because everyone is working as often as they can and it’s still not enough, so the alternative is worse.
When I said last week that the worst was likely behind us, it’s because I think back to when we and other nations faced this situation back in March and April, plus supply chain disruptions and potential full economic collapse. That’s the worst. What’s happening in Belgium now is quite bad, but not as bad as what happened to New York City or to Italy in March and April.
For now, Belgium is going into a six week lockdown as of October 30. Schools are being closed for two weeks, in contrast to England and France where they are being kept open, and I hope they then extend this until December. Also in contrast to Germany’s lockdown, which seems far less severe, although that makes political sense since their outbreak is much less severe as well for now.
I continue to believe that, given the decision to lockdown, the lockdown needs to be as severe and total – and as soon – as possible. Better to do it quickly than to drag things out.
What I have not heard is what the plan is for after the new lockdowns. We know that we can reduce levels of infection via lockdown, but that buys only a little time if the hockey stick curve returns shortly thereafter. So what is the long term plan? What does it take?
This response from the above link is telling: ”Calculations suggest Germany needs to reduce contacts between people by roughly 75% from the current level,” Lauterbach says. “That is incredibly hard if you want to keep schools and most businesses open.” But bars and restaurants account for many contacts while providing only about 1% of Germany’s gross domestic product, making them “kind of the perfect target for pandemic measures.”
That would make perfect sense… if the current level involved life being as it was before Covid-19.
So it’s essentially an admission that even Germans didn’t even take the most basic and efficient of measures to social distance or mask up.
All or nothing. Either do what it takes to drive to zero cases, do what it takes to maintain R0<1 indefinitely, or accept defeat. There are no other options. And if you’re going to do it, do it early, and do it quickly. The link above broadly agrees, and wants to take cases all the way to zero then impose border controls. If politically viable and the vaccine isn’t close, that seems like the least bad option to me. But you have to mean it, or it won’t work.
I continue to be very confused that major European countries are keeping schools open while otherwise locking down, but don’t have anything useful to add on that subject.
Then again, do you know how you know when something is very safe in context? When even one death is reported as news.
If You Can Make It Here, You Still Have to Quarantine Before You Make It Anywhere In Particular
New York had what seemed like a reasonable policy. New York had very low case counts, while many other states had high case counts. If you are travelling from a state with lots of Covid-19 cases, you need to quarantine or get tested, even if you’re returning home.
Last week, Governor Cuomo had to make special exceptions for New Jersey and Connecticut, because cases have gone up so much everywhere that those states would have qualified for quarantine procedures, along with almost every other state. New York itself would have qualified soon enough, if it hadn’t already. The old policy wasn’t indexed to anything, so it clearly no longer made sense.
The new policy is that all visitors except those from adjacent states must take a test before arriving, get a negative result, then come to the state, then within three days get a second negative result, and must provide proof of both tests. If your second test is positive or you fail to get it, you must quarantine for two weeks. Graciously, he will permit us to take day trips to New Jersey, Pennsylvania and Connecticut without getting tested, but everyone else needs to get tested upon return even if they are gone less than a day. Cuomo has also asked everyone to cancel Thanksgiving.
Does this new policy make sense? Is it cost effective?
When someone travels, they go from interacting with one set of people to interacting with a different set of people. Even if both locations typically have similar infection levels, this mixing of different groups is still going to increase the chance the virus will spread. Combine that with what people typically do when they travel, which is to go meet with other people, and that becomes doubly true. Add in that New York, while not doing great, is doing a lot better than most of the rest of the country at this point, and it seems like a strong argument for taking some precautions. But do these particular precautions make sense and are they efficient?
This is obviously not the first best solution. Whether it makes sense depends on what marginal effects dominate, and on the counterfactual.
What is limiting our ability to run tests? If we have an essentially fixed supply of tests that is slowly increasing, then investing in more tests would be good (and New York is good about this at least relative to other places) but we want to allocate what tests we have in a maximally efficient manner. The first test for each person probably makes sense, but giving two tests to everyone who crosses state lines does not seem efficient.
Whereas if we have spare capacity that we could use if we had the willingness to pay for it, then essentially all additional tests are good ideas on the margin. That’s not quite true but it’s close. Anyone who is out there in the world can benefit from the information and the cost is super low. So in this scenario, if you can’t find other places to get those tests used, then by all means use two per person. Same goes if demand for testing creates its own supply over the short to medium term, which on the margin is plausible.
This certainly makes more sense than universal quarantines from essentially every state, and seems likely to both drive testing capacity and be net helpful. What about convenience cost? I am certainly less excited about traveling outside New York if it means getting tested multiple times. It’s substantially annoying. But that’s plausibly also good, because such travel is risky, so taxing it will help balance things. So long as the tax isn’t wasteful, it’s good.
My rough conclusion after a few days thinking it over is that this is as good a policy as we could have plausibly gotten, and it would make sense to emulate it in other states that are doing much better than the country at large.
Limiting Supply Is a Double Edged Sword
It is tempting to mock statements like this one: “Not sure I understand how reducing how late restaurants, gyms & casinos can be open will help fight #Covid19. The virus doesn’t have a curfew.”
The baseline explanation is obvious. If you close them earlier, less people will use restaurants, gyms and casinos, so the risks they contribute will decline. Every time you close something more often on the margin, things improve. Yes, you would prefer to shut them down entirely, but that may not be practical.
But it’s not obvious that this is right. There are plausible circumstances under which this is wrong.
When those running this town decided to shut down the playground over ‘mask non-compliance’ what happened?
(One story is that you caught the no-good people being no good and you successfully punished them, and their suffering will be a Sacrifice to the Gods who will therefore perhaps look upon us with mercy, with no expectation that this makes anyone directly physically safer. Or that this will increase the power of those making this decision, or stroke their egos, or other such explanations, but we’re going to set all that aside for now.)
A plausible story is that they stopped a dangerous activity, and you trade off the safety against the other costs. Perhaps activity moved to backyards.
Another story is that they moved that dangerous activity to other places where it is still permitted, such as the playgrounds in other towns, which are now more crowded and hence got more risky, and also creates a vector for infection to spread from town to town. Or perhaps the activity moved to more playdates, indoors, with an order of magnitude more risk and probably no masks. Or perhaps everyone involved went generally stir-crazy and lost enough sanity points that they started doing various ill-advised things more often.
It all depends on the substitution effects.
The same goes for limiting hours on a restaurant. If you cut hours in half, and people who would have gone at night instead cook for themselves or get delivery, that’s the trade-off you wanted. You’ve reduced risk.
Also, the virus kind of does have somewhat of a (reverse) curfew for restaurants, in the sense that people are more willing to dine outdoors during the day when there is a sun, and less willing at night when it’s the winter in Massachusetts. It’s plausible that time-shifting people is valuable here, or that cutting off the riskier part of their activity and not the safer part could make sense. Or that people’s gatherings at night tend to be more social and risky for other reasons.
The nightmare scenario is that you close all the bars at 10pm instead of 2am, and instead of half the people coming to the bar in the evening and half at night, many of those who would have gone at night instead pack into the place in the evening, and risk goes up rather than down.
The gym very plausibly has this problem, and limiting hours there seems rather nuts. I am guessing there will be a high degree of temporal substitution. If you partially shut it down, then everyone has to come in at the same time and the place gets crowded. You actively want them open 24/7 so people can socially distance. So we should either open all the gyms all of the time, or close all of the gyms all of the time. We often foolishly ‘compromise’ on this because we lack a physical model, and make everything worse.
All or nothing. Half measures only backfire.
In Other News
Huge if true! Researchers claim to have a machine learning system that can diagnose Covid-19 over the phone by analyzing recordings of a forced cough (pdf). They claim sensitivity of 98.5% and specificity of 94.2%, and for asymptomatic cases a sensitivity of 100% (?!?) and specificity of 83.2%. I’m curious to what extent errors in the test are correlated from day to day. This can all be offered at unlimited scale for essentially zero additional cost. So, of course, it will presumably be illegal indefinitely because it’s not as good as accurate as a PCR test and/or hasn’t gone through the proper approval process, and no one will ever use it. Then again, if one were to somehow download or recreate such a program and run it, who would know?
Attempts at alternative diagnostic methods abound. We also learn that Finland’s Covid sniffer dog trial ‘extremely positive’ except that researchers do not seem to have confirmed, at least in the body of the post, that positive results from the dogs correspond to having Covid-19. All I saw from reading is that the dogs give positive results at about the right frequency. Which is nice, sure, but to be useful it really does have to find the actual positives, no matter how positive the feedback is from travellers.
The WSJ reports that Germany is planning to start vaccinations this year, ideally within hours of the vaccine being approved. As you would expect, I very much approve of this, I hope it works out, and I consider it a huge scandal that we won’t be able to follow them within 24 hours. If the Germans approve a vaccine, give me the damn vaccine.
Especially if it’s for Covid-19.
I still don’t have a good story for exactly what happened in Sweden, and as far as I can tell no one else does either. The graphs are profoundly weird and don’t make any sense. The best I can do is a multi-stage story of adoptive behavior that I would never have proposed unless I was fitting to the graph. Not a great option.
Japan using experiments to fill baseball stadium. Japan has dealt with the virus for the moment, so they get to have half-capacity baseball stadiums. Now they’re looking into whether they can do better than that, by running experiments and gathering data on airflow. Here in America, the NBA used sports as a justification to innovate superior testing and isolation procedures, which we hope can then be used to help the rest of us. In Japan, baseball gets to do the same. I wonder what other experiments we could run using this trick to end-run around civilization’s ban on experiments and data gathering.
Antivirals work best if given early, before you know for sure that you need them. The vulnerable thus face the Catch-22 of not being able to get antiviral meds before they are in the hospital/ICU, because they’re not sick enough to justify it, and then when they end up there because they didn’t get the medication early, are told it is too late because the medication would no longer work. Here is one such story. I have not verified this.
White House Advisor Scott Atlas has said some rather brazenly false things about Covid-19 and the course of the pandemic. It is not my place to say whether he knows they are false, or whether he cares whether they are false, or even thinks the question is meaningful. Either way, given his position, his statements risk doing great harm. I understand the desire to push back.
But destroying more of what remains of academic freedom to do so is not the way. Academic freedom questions arise on campus over COVID-19 strategy conflicts paints a chilling picture of how people on campus are currently thinking about such questions. Consider this quote:
[Spiegel] said, “There are limitations to academic freedom. What you express has to be honest, data-based and reflect what is known in the field. If you are going to claim academic freedom, you had better be academic, as well as free.”
If, in order to claim academic freedom, you have to say things that reflect what is known in the field, then what is the point of academic freedom? Being free to agree with what everyone already thinks is better than not being able to say anything at all, but not by that much. Only being able to say ‘data-based’ things would in many cases not be much better, especially given who decides what is data-based. Censorship in general seems to rapidly be on the rise, in academia, on social media and elsewhere. If left unchecked, this will not only hit the outgroup, and it will not end well.
This seems like a wise framing of how off the rails our (lack of) thinking has been this whole time regarding what is appropriate and ethical:
Reminder that “Much of our understanding of other coronaviruses comes from challenge trials done in the UK in the 1960s” back when we still were capable of doing such things.
One risk with a vaccine is that if the vaccine is only somewhat effective, and it causes mask usage to decline, it could end up not only not helping but making things worse. As with many such ‘papers’ this is a basic mathematical truth rather than some new finding, but important nonetheless, especially if non-vaccinated people also stop taking precautions. I expect to be able to deal with these types of problems, but there’s definitely risk there.
New study estimates 30,000 confirmed cases and 700 deaths from Trump rallies. Which would (among other things) be a CFR of over 2%. Also note that this effect would persist, as those people in turn infect others, so those 700 deaths should recur until we get things under control. All effects that make things worse are deadlier than they look until control systems set in. Effect size seems plausible to me. I would have liked to see more attention on the indoor vs. outdoor distinction, as there were three indoor rallies in their sample.
This study casts doubt on the effectiveness of contact tracing. More precisely, it casts doubt on the effectiveness of such tracing in San Francisco. It was hopelessly slow, waiting 6 days after symptoms to contact potential other cases, and failed to identify many new positives. I think this says a lot about our state capacity and ability to coordinate around such tasks, and very little about contact tracing beyond our inability to implement it usefully. As long as we are more concerned with privacy and voluntary cooperation than pandemic containmentent, and don’t actually want to do this for real, it won’t work. A shame.
I neglected last week to talk about how risky it would be to go Trick or Treating and whether doing so made sense and how to do so responsibly, both as a parent or as a giver of candy. I didn’t think about it. The answer seems obvious, which is that unless you’re doing it in a large group in an apartment building, all you’re doing is walking around outside and being given individually wrapped candies, so it’s obviously fine to leave out a bowl of candy and take from the bowl. Divia confirms this was how things worked in her area, my wife confirms the same in Warwick. I’m not worried about trick or treating at all. If anything, it’s a relatively low-risk way to stay active and avoid going stir crazy, and I’m sad I wasn’t able to join.
What did worry me were reports of adult indoor parties on Halloween, which fell on a Saturday night at a highly stressful time. I saw a number of them, but it’s hard to translate that into a good sense of how common they were. This is the one night many young adults and teenagers consider themselves to have a pass to act irresponsibly and there’s no reason to think this wouldn’t apply to pandemic precautions as well. Even the Surgeon General’s kid doesn’t get it. One could hope that the holiday would at least encourage mask compliance.
Paul Romer has yet another column on how crazy it is we don’t do massively more testing.
All I Want For Christmas Is (Still) a Covid Vaccine
Part of the story of why it’s going to be a while is that people like Speaker Pelosi are actively getting in the way via refusing to accept an approval in the UK as good enough for us. It would be very difficult to overstate my outrage that this is happening, and I really hope this is pure hypocrisy that will be reversed by coincidence on January 20.
In any case, it may be time to reset expectations on when we’ll get a Covid-19 vaccine.
I’m not sure how much of a reset is being called for here. My understanding was that October was always about the best-case scenario but required a lot of things to go right slash it would have been a political move by the administration, and something more like December was more of the hopeful case where still things mostly go right. The reasons to be optimistic are that there’s lots of irons in the fire only one of which needs to work, and there’s huge incentives pushing on everyone involved to get this done.
Like everyone else, I did get my hopes up somewhat, cause it’s been quite the long slog, but the timeline we are supposed to reset to does not sound that different. The article talks about asking for emergency authorization in mid-November for Pfizer, with Paul Mango of Health and Human Services expressing hope we can start with our most vulnerable by the end of the year, finish that leg by January, and everyone who wants it by March or April. That seems pretty great if it happens.
We are warned that we ‘may not get a vaccine by the end of 2020’ but that’s a warning that’s been loud and clear the entire time. So what’s the expectations reset here? And what has unexpectedly or unpredictably gone wrong, given the results themselves all seem promising?
Another way to put this is, there have been delays off the engineering schedule, but only those who lack engineering experience expect things to happen according to the engineering schedule.
Particular trials are behind schedule because they were paused or not enough people were infected, but are those things a surprise? Should we have expected anything else? Were these problems inevitable? I also felt the need to double check one other question: What exactly happens when these trials are paused, anyway?
The only thing that happens when a trial is paused is that they stop recruiting new patients. There is no reason to stop following the people already in the trial, you can’t undo a vaccination, and doing only part of a vaccination is not advisable. So pausing a trial for five weeks will slow it down if it hasn’t reached its ideal size, but presuming one is looking for a critical mass of data, it will be much less than five weeks of delay.
This also suggests that it is vitally important, when starting a trial, to get everyone treated as rapidly as possible once you start treating anyone. Otherwise, every time even one person in any arm of the trial has any serious medical issue, which is likely to happen even if the drug is a sugar pill, you end up paused, perhaps for a long time.
The second problem the trials are running into is that not enough people in the trials are catching the virus, which I assume refers to the control group.
Which raises an obvious question. Infections are clearly on the rise. If you’re not getting enough infections now, what was the expectation? What went wrong?
The pauses are getting in the way, but are far shorter than the delays and at least somewhat expected, so that’s at most a minor explanation.
If anything there should be substantially more people infected in the control group than one would have expected. There were previously concerns that cases were down and that (as welcome as it would have been) would interfere with gathering data. The opposite happened, so what’s the problem?
The trials were too small. There were some reports of problems recruiting for the trials, especially among desired subgroups. This of course is partly because it’s illegal to pay participants, but the importance of these trials is off the charts and a substantial portion of people I know would have volunteered if asked. It would not have taken much effort to find more volunteers.
The most basic explanation is ‘you should get many times more people than you need in order to finish quicker than you expect, and then double it again’ and they instead tried to get ‘enough to expect to finish on time’ and then stuff happened.
Or, rather, the main thing didn’t happen much, and this took them by surprise when it really shouldn’t have.
The Old and the Cautious
My guess is a key thing that happened is that they failed to anticipate how careful their trial participants would be compared to the general population.
A point I have emphasized time and again is that most Covid risk comes from doing stupid stuff. Not wearing a mask, indoor gatherings including indoor dining, massive packed political rallies, college students being college students, that sort of thing. There’s also some jobs that require repeatedly taking substantial risk, but mostly the statistics I’ve seen suggest that proper mask and barrier precautions work wonders even then. Each of several factors in an activity change the order of magnitude of risk taken. Those changes multiply together. Many people are doing radically fewer activities with people they don’t live with while taking lots of precautions, while others act as if everything is normal.
The people who take the stupid risks take them repeatedly, so the people you interact with when taking stupid risks are stupidly risky people to interact with, multiplying risk again.
If you do a study with people who care enough about not catching Covid-19 to seek out a vaccine trial, most of your sample is not going to react to maybe being vaccinated by throwing caution to the wind. They’re going to be almost as cautious as before, because that’s the type of people who sign up. The drug companies intuitively thought they’d get an infection rate not too far from population baseline, and (I am guessing) instead got one radically lower.
On reflection, like everyone else I want to see the treatment group and know whether the vaccines work, but I am also remarkably curious about the control group. The control group is not a representative sample of the population. It is a sample of a very interesting subpopulation. Let’s find out what types of activities these people participate in and how often by asking them, and let’s compare their infection rate to the general population adjusting for various known factors, and let’s run the whole correlation matrix and see what happens. If we can’t run studies otherwise, we have to take advantage of every opportunity we can get.
On Herd Immunity (A Version of This Likely Will Become Its Own Post)
Last week I had an influx of people reading my weekly column for the first time, by way of Twitter outrage and the inevitable Streisand Effect. Lots of people were pointing at this supposedly wrong and awful thing to say how wrong and awful it was. They pointed out an important misquote which I corrected. Mostly it was a lot of ‘experts/doctors/Fauci say X and he says ~X so he’s wrong and dangerous’ including after it became clear that once the quote was corrected I locally agreed with Fauci.
Whole event was stressful at an already stressful time for all of us, but did double the post’s readership and correct an important error, so overall I can’t complain.
The only other substantive complaint was that several sources rightfully challenged my herd immunity claim. It is quite a bold claim, a new reader wouldn’t know how I was justifying that claim as I hadn’t gone over my reasoning at least for a while, and in full perhaps ever, at least in terms of putting it all together at once.
Time to do that now, as promised.
Early in the pandemic, I did an analysis post called On R0. Looking back on it now, I see a bunch of stuff I got wrong, but I still agree with the three central points of the post absent substantial mutations of the virus.
The first central point is that if everyone lives their life as if Covid-19 does not exist, we know R0 started out somewhere between 2.5 and 4 in most places, perhaps up to 8 in a few like New York City. If we reduce risk by 75%, we will suppress and potentially eventually eradicate Covid-19 in all but a few places. In those few places, we’ll need more.
The second central point is that there are a lot of relatively cheap and available ways to cut those risks by 75% or more. Most people I know have cut their risk by 90% or more, before considering that those around them have also mostly done the same.
The third central point is that different people have radically different risk levels, that the riskier people are taking most of the risks, frequently with each other, while others have radically reduced their risks, and that the risk takers will mostly get infected first.
Combine those points and it seems obvious to me that by the time you get 50% infected, you’re going to reduce effective risk by more than 75%. Even with no other changes, that’s a victory condition for most places, and there will doubtless be some amount of behavioral change. We are not going to shake hands as often as we did, or be quite as up close talking, and will be more wary if we start coughing and so on, even if masks mostly fall out of favor once things die down. My conservative guess is that the needed number is more like 35%.
The classic objection is to point to the classic SIR model – susceptible, infected, recovered. This model treats everyone as identical people who take identical risks identically often with identical others completely at random, and are all equally susceptible to infection. That model is, upon reflection, either a toy model upper bound to be used in the spirit in which it was created, or obvious nonsense if taken seriously.
The even stronger objection is that you need to infect enough people so that the most risk taking communities have R0 below 1, but then treat infection as if it is evenly distributed. This isn’t a straw man, this happens periodically and happened again last week. The conclusion is then that you need e.g. 90% infected. But this is both lacking one’s cake and not eating it too. If different groups are differently risky enough that it matters, then the infections seek out the risky first.
Thus, the first part of the explanation is that my reasonable range for the original herd immunity threshold is between 25% and 50%. What we’ve seen since then seems compatible with this range. On first principles I would have put substantial weight on the lower range here or even lower, but the evidence since then seems to reject the lower end of my range. It also seems more consistent with the higher end of my range than it would with higher numbers, as one area after another peaks relatively quickly once spread gets completely out of hand, almost no matter what policies are chosen, combined with the antibody test data suggesting that infection rates are much higher than the PCR test results alone.
The second part of the explanation is that there are a lot more cases than positive tests. In most places, I believe that we are detecting at most 25% or so of cases in most places, and that number used to be even lower. The higher the positive test rate, the higher the percentage of cases we are likely missing. As of writing this about 2.8% of the population has tested positive, but I am guessing more like 18% of the population was positive at some point. This roughly matches the machine learning source I was using (which is no longer updating) and other similar sources like this one. There is of course disagreement on the exact number, but mostly I see people with broadly similar guesses and people who effectively treat positive tests and infections as identical. I see few in between.
In my model, that 18% is the only reason cases are only increasing at something like 10%/week instead of going full hockey stick in a similar way to Europe. Over time, more people become immune, but also over time people are taking on more risks, as fatigue sets in and now as the weather gets colder. The two effects work to offset each other, and people adjust their behaviors for the death rate, which combine to create a control system.
To figure out how many deaths would be required to hit herd immunity, we need to know two things: How many must be infected, and the infection fatality rate for new infections. If 18% are already infected and the threshold is at most 50%, then we need 32% additional infections out of 331 million people, or about 106 million new infections. What is the IFR?
We don’t have great data, the same way we don’t have great data on many other things, and for the same reasons. What we do know is that the IFR has dropped dramatically. Early in the pandemic, I was estimating 0.6% in the absence of medical system collapse, and using a 1% IFR for my calculations to be conservative. At this point, I think the upper bound is 0.4% or so, and my best guess is around 0.2%.
If the IFR is 0.2% and we need to infect 106 million people, then we would need just over 200k deaths from here to reach 50% infected, which puts the cap safely well under 500k deaths. If the IFR is higher and remains 0.4%, then it would be double that, and if the necessary infected were on the high end we would go somewhat above 500k deaths to around 650k. That seems like the worst case scenario absent medical system collapse or fading immunity, and my median estimate – again, assuming there isn’t a medical system collapse – is that this ends around 400k American deaths unless we get a vaccine in time to improve that.
An intuition pump might be that I think we are roughly 1/3rd of the way through in terms of infections, but the death rate has been at least cut in half, so that later two thirds shouldn’t kill more people than have already died.
That’s a lot of deaths, and deaths are really bad! It also would mean a lot of suffering. If we have a practical way to cut that down to 300k, it’s worth a lot to do that. I just don’t see any sign that we have a practical path to that outcome.
The new mutation throws a wrench into all of this, potentially driving the necessary thresholds much higher. If the new virus is twice as infectious in the sense that under typical conditions an infected person now infects an average of 8 people rather than 4, then we have to cut risk by 88% instead of 75%. That’s a lot harder.
If I had to make a rough guess, I’d say that it’s probably not as bad as that. I haven’t seen any clear estimates, but Europe is now almost entirely dealing with the new strain as per the Financial Times and other sources, and looks like it had an R0 between 1.2 (the most visible outside estimate I’ve seen) and 1.35 (my eyeballed ballpark estimate for France) before its new wave of lockdowns, despite widespread completely irresponsible behaviors. Before that, governments seemed to be going for a balance to keep R0 at or just below 1 (in some cases like Cuomo here in America we even hear goals just above one, which is madness and completely innumerate) and we didn’t see anything approaching eradication. If anything, until things were well out of control, behavior was growing less responsible rather than more responsible. Thus, we can presume that the previous R0 was very close to 1.
Take that all together, and my guess as to the effective practical increase is that it is on the order of 20%-35%, so we’ll need something like an 80% reduction rather than 75% to put the whole thing to bed. That’s a huge problem when it initially interacts with an ill-prepared control system, but still seems like a target that is well within range of reasonable measures and would be reached not that long after 75% through immunity.
This is definitely not an argument that proves we should stop trying to contain Covid-19 and ‘go back to normal’, or rely on herd immunity ‘strategy’. If we stopped trying to contain it on all levels, it seems likely we would collapse the medical system, and we would lose many more people and politically likely be forced to do more lockdowns that would lead to severe damage on many fronts. Also, our preventative measures are likely themselves also reducing the death rate in other ways.
On the margin, however, it is informative of our choices, both individually and as a group. It informs us of the costs and benefits of different choices. If we are going to pay a massive price on many levels to try and do better than the scenario outlined above, we need to know the magnitude of the benefits, and compare it to the magnitude of the costs.
It is also entirely possible that I am wrong. I welcome challenges to the model (in both directions!), so long as they are not another iteration of ‘but experts say’ or ‘you’re not an expert’ or reiterating standard SIR without arguing why my objections to it aren’t valid. To the extent those objections have content, I’ve absorbed and responded to that content already.
If I am making a well-calibrated estimate given everything I know and believe, half the time I’m going to be too optimistic even after adjusting my estimate for such worries. If we lose more than 500k Americans before this is over without medical system collapse or a lot of reinfections, that would surprise me but not shock me. It would likely be because the IFR is somewhat higher than I think it is going forward, combined with us increasing our risk taking more than I expect, or if the mutation of the virus is a bigger deal than I’m estimating. I am not at all saying that this would be a Can’t Happen. I will however be shocked if the medical system does not collapse, reinfections are not a major factor, and we then see 750k deaths or even 1mm deaths.
Of course, we will only know the answer if this scenario happens. That seems increasingly likely, but it is far from certain.
The Good Doctor
Given what happened last week and my accidental misquoting of Dr. Fauci, I should explain how I see Dr. Fauci’s role in all this.
I believe Dr. Fauci mostly has an unusually accurate picture of what is happening, and that he is doing his best to contain the pandemic given his position and the tools available. He’s been doing his best to maintain public health while serving under several presidents. He has had a truly thankless job this time around, forced to fight constantly with the administration over even basic facts of the situation.
Mostly he’s been fighting the good fight. He also has a way with words. There’s a reason the public trusts and likes him so much.
That doesn’t mean we agree on everything, or that I always agree with the things he claims or suggests.
There are several issues.
The first issue is that Dr. Fauci is operating primarily on Simulacra Level 2 with some consideration for Level 1 – he tries to provide information that will cause us to change our perceptions of reality and thus alter our behavior in ways that will save lives, and worries some about whether his information is misleading or false because he thinks credibility matters too.
While not quite where I would want him to be, that is a huge improvement over the bulk of people in power, who are operating mostly on Simulacra Level 3 or even Level 4, and is why this section is titled The Good Doctor.
He has shown he is willing to tell what he feels are white lies in order to change the public’s behavior and save lives. I emphatically would not have done this in his place, but I am not judging. The ethical questions involved are difficult. In his position, most others would do the same. In practice, I think the lies he and others told about masks were massively destructive in a way that was knowable in advance, but I do think that he lied with the best of intentions.
The whole projection of 400,000 deaths by the end of the year was another (but less egregious and not very harmful) similar case. I believe I know what he’s doing and why he’s doing it, and we can disagree about whether it matters that the numbers don’t add up unless you stare at them in exactly the right way. In a world in which he’s up against an administration (that he’s nominally still working for!) that tells a different order of magnitude of lies in both quantity and severity feels relevant here as well.
Thus, when Dr. Fauci makes a statement, I have to hear it in light of his primary motive, which is to cause us to act responsibly and save lives. It makes sense to worry that he might tactically join the Doom Patrol in the context of a vaccine, if he was worried it would cause us to let our guards down too far too soon, and he felt the need to lay groundwork to prevent that.
Still, he didn’t do it last week, and I wasn’t as suspicious as I should have been when it looked like he was doing it. Yes, he’s willing to mislead when he sees it as necessary, but this particular claim didn’t fit the pattern. That’s why I felt it was important! It seemed like he was going full Doom Patrol at Level 3 on this issue, which would have been a change from his usual actions. Thus, I noticed that this was an important change to notice, and that would require pushback and attention, but failed to notice that this also meant there was a good chance it hadn’t happened. I should not only have verified the quote more carefully, I should have been extra suspicious. I wasn’t, I need to do better, and that’s on me.
The second issue is a disagreement between our models. Dr. Fauci probably disagrees strongly with my model of future herd immunity, through some combination of disagreement over how many are infected, and disagreement over the heterogeneity effects. I believe these disagreements are genuine, but also that not much effort is being made to consider models like the one I outline.
The other disagreement we have is that Dr. Fauci (as far as I can tell) believes in the general wisdom of medical ethics and procedures, and in all the barriers we have that stop people from doing things. I don’t.
That’s the context in which I evaluate Dr. Fauci and his statements. I want him to keep his job. Of all the major authorities, his statements are the most credible, both in terms of his expertise and his honesty, but we still have to evaluate his statements in light of the fact that he is primarily telling us what he feels we need to hear in order to stay safe, and only secondarily telling us what he believes.
And, of course, sometimes and on some things, we will disagree.
Paths Forward
This was a super long weekly post because there was some overhead from last week to deal with, and the opportunity to flesh some of it out was a welcome distraction. There’s still a lot to do.
This week I gave a presentation of my updates on Covid-19 in a rationalist town hall. It ended up taking an hour, and there were tons of things I left out. It is high time I wrote up a summary of my current model and key things to know. If I can find the time and focus, I hope to turn that presentation and my thoughts above into a post or series of posts that can act as reference/entry points.
On a practical on-the-ground level, it’s getting steadily worse out there, and is unlikely to turn around in the next month or two. The best case short term scenario is that it soon stops getting worse in terms of real infections, while positive tests and deaths keep rising for a while due to lag. To the extent that infection risks are worth taking, they are not going to get less risky for a while. If you have Thanksgiving or Christmas plans, think carefully about the risks involved, and consider cancelling your plans or at a minimum reducing the size of your gatherings.
It is going to be ugly out there. Stay safe.